Dr O’Brien is the founder and CEO of TOB1 Consulting. He is a senior executive within the healthcare industry with more than 30 years experience as a CEO & main board Director. He has successfully taken several cardiovascular, vascular access, orthopaedic, anesthesia and hemodynamic monitoring technologies from the laboratory bench to full scale manufacture & commercialisation in major markets. He founded the LiDCO Group Plc at St Thomas’ Hospital, London to develop and commercialise digital minimally and non-invasive hemodynamic monitoring technology, now used at many sites throughout the world. LiDCO Group Plc was acquired by Masimo in February 2021.
OFIS® is a trademarked acronym short for Optimising Fluid In Surgery and is the name of the platform technology that TOB1 are developing for the modelling of the impact of intravenous administered fluid on the vascular volume, hemodynamics and body tissue fluid compartments in patients undergoing major surgery.
Fluid administration is needed to establish and maintain an adequate blood volume, despite vascular vasodilation, blood and fluid loss, capable of maintaining the venous blood flow return gradient. This, in turn, means that the heart can effectively pump sufficient oxygenated blood (cardiac output) to the body to ensure adequate blood pressure and oxygen delivery is available for tissue beds to perfuse properly and maintain cell viability.
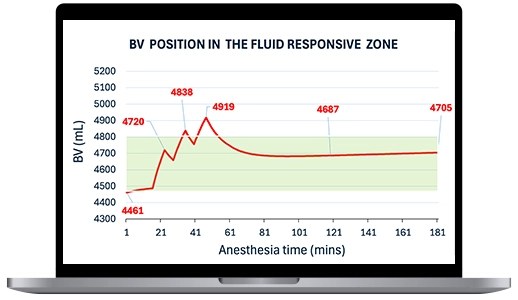
The administration of anesthetic drugs to patients undergoing surgery causes profound vascular changes and impairs cardiac efficiency. The dilation of the blood vessels means that venous return of blood diminishes and the blood flow and blood pressure fall. Extra fluid is often required to re-fill the expanded capacity of the vascular compartment. When required, this volume is usually delivered after anesthetic induction as one or more rapidly administered restorative fluid challenges to “optimise” the circulation blood volume and associated blood flow. Following the initial optimisation the goal is then to maintain the “optimised” blood volume by administering a continuous maintenance fluid volume at a set rate that ideally would match blood and other losses of fluid from the blood stream during the surgery.
Fluids are pharmaceutical substances; they exert important physiological effects and therefore should be considered as “drugs.” Fluid therapy is an evolving but still imprecise clinical exercise. Practice is still, largely based on broad assumptions, incomplete data and individual preferences. Fluid therapy is widely practiced as a mainstay therapy in many areas of human medicine, however fluid therapy is not always benign and can cause harm through fluid over or under load, both increase patient morbidity and mortality rates and hospital bed use.
Existing fluid management parameters (fluid responsiveness SVV%, PPV%, PVI; fluid response ∆SV) are limited in their precision and are indirect indicators of blood volume adequacy. Although these have been useful, there remains a need for further information regarding the underlying blood volume changes that occur after anesthetic induction and subsequent IV fluid administration. The pharmacologic and pharmacokinetic properties of crystalloids and colloid fluids are very different and must be considered when planning fluid administrations to both restore and maintain blood volume. The measurement of the blood volume changes following fluid administration has always been an ambition, but methods to measure blood volume were cumbersome and not of practical use in fast moving dynamically changing surgical settings.
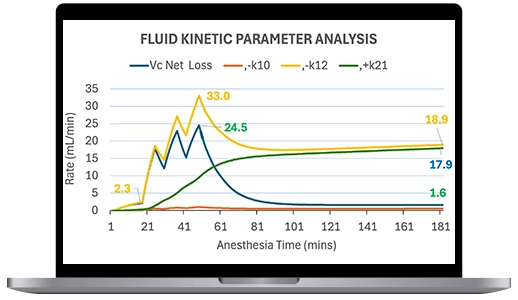
Drug kinetics (pharmacokinetics) describes how the body deals with an administered drug, quantifying its absorption, distribution, metabolism, and elimination phases. It has been possible to fit IV administered fluid dilution data to an equation that describes fluid distribution and elimination with use of two, and for longer interventions, three compartment volume models. The approach taken by the OFIS® computer model kinetic analysis describes the both the peak effects, distribution and clearance of intravenously infused fluid boluses and maintenance fluids.
Volume kinetic models are potentially very useful tools to better understand fluid distribution, elimination and overall impact on the blood volume. They have potential to be used for designing and implementing more efficient fluid therapy protocols. These models are flexible and can be adapted to fit the kinetics of different fluids (colloids and crystalloids), clinical situations (body position, minimally invasive /robotic surgery) and locations of use (perioperative, intensive care, emergency room).
Currently crystalloids are preferred over colloid for fluid challenges. Using existing technology to judge the best dose and rate of infusion to achieve and maintain an optimal hemodynamic and oxygen delivery impact is more problematic than when using colloids. Their impact on the BV is smaller and with successive fluid challenge administration becomes unpredictable*. In the future IV fluid dosing could be guided by fluid pharmacokinetic analysis adjusted to the operative conditions/stage and type of fluid selected. Continued administration of IV fluid to subjects that are fluid non-responders will result in unnecessary increases in tissue fluid and eventually potentially damaging third-space losses. Hitting the sweet spot for fluid administration will be much more likely when kinetic modelling is added to existing dynamic measures of fluid responsiveness and the monitoring of hemodynamic parameters such as cardiac output and oxygen delivery.
*Hahn RG, O´Brien T. Attenuation of the plasma volume response to crystalloid fluid used for goal-directed fluid therapy. Ann Intensive Care 2025; 15: 83.
Yes, there are many publications! In terms of reference centres Professor Robert Hahn at the Karolinska Institute in Stockholm has been the most important key researcher in this field. In 1990 he pioneered the concept of using “volume kinetics” analysis, through the adaptation of pharmacokinetic drug models to infusion fluids.
Following Prof. Hahn’s introduction of the idea for “volume kinetics” analysis, this area has been the subject of over 100 publications and multiple PhD programs. Prof. Hahn has published many scientific papers in peer-reviewed journals and edited 4 books of fluid therapy in the perioperative setting.
We are pleased to say that we are working in close collaboration with Prof. Hahn to develop educational and clinical applications of fluid kinetic analysis using the OFIS® platform. Dr O’Brien is a co-author with Prof Hahn16 on a research paper with important clinical implications as to how kinetic analysis can suggest improvements to the method for fluid challenges using a variety of solutions. A second paper17 has been written that readdresses the methodology of the fluid challenge by analysing a unique data set of blood volume and stroke volume changes following fluid challenges under anaesthesia.
See below for a list of useful papers dealing with volume kinetics:
1. Hahn RG, Bergek C, Gebäck T, Zdolsek J. Interactions between the volume effects of hydroxyethyl starch 130/0.4 and Ringer’s acetate. Crit Care 2013; 17: R104.
2. Hahn RG. Arterial pressure and the rate of elimination of crystalloid fluid. Anesth Analg 2017; 124: 1824-1833.
3. Hahn RG. Understanding volume kinetics. Acta Anaesthesiol Scand 2020; 64: 570-578.
4. Hahn RG, Drobin D, Li Y, Zdolsek J. Kinetics of Ringer’s solution in extracellular dehydration and hemorrhage. Shock 2020; 53: 566-573.
5. Hahn RG, Drobin D. Model-predicted capillary leakage in graded hypotension; extended analysis of experimental spinal anesthesia. Acta Anaesthesiol Scand 2021; 65: 1313-1319.
6. Hahn, RG, Olsson J. Diuretic response to Ringer’s solution is normal shortly after awakening from general anaesthesia; a retrospective kinetic analysis. BJA Open 2022; 2: 100013.
7. Hahn RG. Accelerated lymph flow from infusion of crystalloid fluid during general anesthesia. BMC Anesthesiol 2024; 24: 119.
8. Hahn RG, Zdolsek M, Gunnström M, Hasselgren E, Zdolsek JH. Diuretic responses to Ringer’s solution and 20% albumin at different arterial pressures. Physiol Reports 2024; 12: e70069.
9. Hahn RG. Do volatile anesthetics depress urine output? Anesth Intensive Ther 2024; 56: 185-193.
10. Hahn RG. Sequential recruitment of body fluid spaces for increasing volumes of crystalloid fluid. Front Physiol 2024; 15: 1439035.
11. Zdolsek M, Hahn RG. Kinetics of 5% and 20% albumin: A controlled crossover trial in volunteers. Acta Anaesthesiol Scand 2022; 66: 847-858.
12. Balan C, Boros C, Bubenek-Turconi SI, Hahn RG. Volume kinetics of Gelofusine 4% during vascular surgery. Clin Pharmacokinet 2025; 64: 599-610.
13. Dull RO, Hahn RG. Hypovolemia with peripheral edema: What is wrong? Crit Care 2023; 27: 206.
14. Dull RO, Hahn RG, Dull GE. Anesthesia-induced lymphatic dysfunction (review). Anesthesiology 2024; 141: 175-187.
15. Hahn RG. Volume kinetic analysis in living humans; background history and answers to 15 questions in physiology and medicine. Fluids 2025; 10: 86.
16. Hahn RG, O´Brien T. Attenuation of the plasma volume response to crystalloid fluid used for goal-directed fluid therapy. Ann Intensive Care 2025; 15: 83.
17. O’Brien T , Hahn RG. Revisiting the fluid challenge and stroke volume optimisation in patients under anesthesia in surgery, Submitted for publication.
Anesthetists are still looking for additional support with the tailoring of the administration of IV fluids. The idea for fluid kinetic analysis has been around for a while now but has only come of age very recently. More precise and detailed (2 and 3 compartment) mathematical models for the pharmacokinetic modelling of IV fluid are now available. These have now been adapted to model the varying fluid requirements of surgery patients who experience rapid vascular compliance changes and fluid shifts that influence IV fluid redistribution and elimination during major surgery.
Applying fluid volume kinetic analysis to individualise and target fluid administration to both achieve and maintain a specific blood volume and better interpret the impact of fluid challenges and maintenance fluid rates is novel. TOBI has granted patents and has filed follow-on patent applications that cover claims for these methods both as educational applications and for use in patient monitoring devices.
Initially we are focussing on producing publications and public resources that increase the understanding of the importance and potential clinical utility of blood volume monitoring by use of computer pharmacokinetic simulation. Blood volume is one of the most important parameters missing from fluid management today. The Company’s first products will be interactive, models of the circularity (blood volume) and hemodynamic response to IV fluid administration in patients under anesthesia in surgery.
Our two first products – OFIS® Trainer and OFIS® Trainer+ are solely designed for educational use. OFIS® Trainer (patents granted & pending) will be the first interactive fluid model for simulation of the compartment volume changes following IV fluid challenge bolus and maintenance fluid infusions in patients under anesthesia.
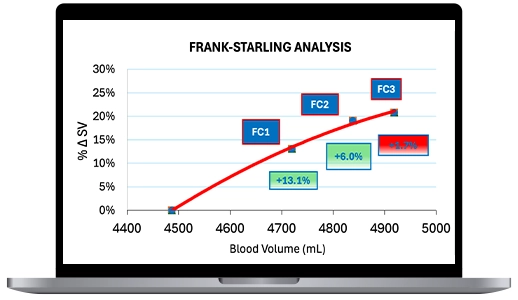
The OFIS® Trainer+ adds Frank-Starling simulation of the hemodynamic (stroke volume) impact of a fluid challenge procedure. The fluid pharmacokinetic model determines the fluid challenge volume to achieve a defined blood volume change.This analysis uses a novel and proprietary method (patent applied for) of identifying a pre-load dependent and a pre-load independent blood volume range.
OFIS® Monitor program. Ultimately there are many potential clinical uses for the OFIS® technology. For example, our simulations suggest unexpected and novel ways of using the different pharmacokinetic properties of different types of fluids to more effectively achieve and maintain the blood volume during surgery. These novel protocols will need to be validated in prospective clinical trials. If proven beneficial OFIS® computer simulation could be integrated into existing monitoring systems and clinical practice.
Sign up with your email to get notified of our latest news.